A wake-up call to health inequities from nationally recognized expert in health care policies
In a session that is a collaborative effort between Spectrum Health Lakeland and the Berrien Community Foundation health policy expert Daniel Dawes tells how political decisions and public policy create community conditions that harm our nation’s health unless people take action.



“We have to wake up!” says Daniel Dawes, JD, executive director of Satcher Health Leadership Institute at the Morehouse School of Medicine.
Dawes is recounting a story from his childhood, attending church with his sleepy brother, Patrick. The preacher’s call to wake up was effective on his young brother, alerting him to the importance of the call. The boys sat up and listened.
On Nov. 17, 2021, the audience, however, are the listeners at a Zoom event, presented by Community Grand Rounds, a collaborative effort between Spectrum Health Lakeland and Berrien Community Foundation.
Lynn Todman, PhD, Vice President Health Equity, Spectrum Health, hosts the event.
Dawes is nationally recognized in health care law and policy, leading many efforts to address health inequities affecting vulnerable and underserved populations in the United States, Todman says as an introduction.
Among his many achievements, Dawes founded and chaired the largest advocacy group focused on developing comprehensive law to restructure the health care system and address inequities. He also helped shape the Affordable Care Act and is the author of two ground-breaking books: Political Determinants of Health and 150 years of Obamacare.
“The point of my story about the preacher’s wake-up call,” Dawes continues, “is that sometimes we all need a wake-up call. This is our fourth awakening in the U.S. on health inequity. The pandemic has been a dark time, a racial and social reckoning.”
Dawes explains how political decisions and public policy create community conditions that harm our nation’s health. He reveals how such decisions and policies result in polluted water and air, unreliable transportation, unsafe neighborhoods, unhealthy food options, low incomes, and other conditions leading to health inequities.
“I believe that we’ve reached a point in our society where the main causes of health inequities are actually one and the same with the main drivers that continue to perpetuate these inequities,” Dawes says. “By that, I’m referencing the political determinants of health. Most individuals are at least vaguely acquainted with the social determinants of health and their role in our day-to-day lives. The conditions where we are born, live, learn, work, play, and pray, are the basis for many of the health inequities that plague our society. However, the social determinants do not tell the whole story and fall short of providing a plan for addressing the inequities.”
The United States is currently ranked 43rd in life expectancy in the world, Dawes reports. Yet we consume more than half of the world’s health care resources. Life expectancy is falling for all Americans, but more so for marginalized populations.
“If we look at only white America, we rank 50th in life expectancy worldwide,” he says. “If we look at Black America, we rank 103rd, but Native American ranking is 143rd.”
To illustrate how health determinants in our society impact individuals, Dawes shares another story—this one about a fictional character, Jessica, a 19-year-old single woman who has experienced several miscarriages, who then gives birth to a premature baby weighing only three pounds and found to have toxins in his blood.
“Where has the system failed her?” Dawes asks as he goes on to tell of a low-income community where health centers are closed, educational resources are limited, job opportunities are nearly nonexistent except for those paying minimum wage (not livable wage) salaries or without benefits. Zoning laws can leave a community without protections from substandard water sources, along with other factors that affect the health of community members like Jessica.
“Marginalized groups live in precarious situations, falling through the cracks as society erects barrier after barrier,” Dawes says. “The political determinants, on the other hand, truly get to the root cause of health inequities and their entrenched nature in our society. These determinants refer to the upstream factors in our system which create, sustain, or influence the social determinants which, in turn, lead to the downstream impacts that we see as health inequities among under-resourced, minoritized, and marginalized population groups.”
Dawes next took up the original sources of these inequities, using the illustration of a tree with wide and deep roots. Those roots, he says, reach back to health policies established in 1865 with the contentious passing of the Freedom’s Bureau Act.
The Act included health resources for minorities, but government branches argued over this part of the Act for nearly two years, even as President Abraham Lincoln urged compromise. Medical resources were stricken from the Act and health policy addressing marginalized groups wouldn’t come up again for 150 years—with the Affordable Care Act, which includes 62 provisions that elevate care for the marginalized.
“The Affordable Care Act made significant headway in helping individuals understand the impact of health equity on their daily lives,” Dawes says. “It brought the topic out of the classroom and to the dinner table. And that, I believe, is going to be one of the single greatest lingering effects of the ACA.”
“Every social determinant of health that you can point to, there was some preceding legal, legislative, policy, or regulatory decision that resulted in the aforementioned social determinant,” Dawes continues. “By understanding, and more importantly, harnessing the political determinants of health that play an outsized role in our society, we can begin to truly address and ameliorate the downstream social determinants of health that manifest as health inequities.”
Policies affecting health inequities today, Dawes says, can be found in discrimination against various ethnic and racial groups, the disabled, Native tribes, immigrants, and others. How we address climate change, poverty, redlining and other forms of segregation can all have an effect on health equity.
“Where you live matters,” he says. “While one neighborhood in Grand Rapids has a life expectancy of 65.6 years, the neighborhood adjacent to it has a life expectancy of 90.8 years.”
Bringing the issue of health inequity home to West Michigan, Dawes advises how health care organizations such as Spectrum Health—and all such organizations—can improve health care for all.
“The two most important things that health care organizations can do are to, first and foremost, be aware of the power and influence they wield, and second, to prioritize pushing for a more healthy, equitable, and inclusive future. Simply by virtue of our health care system, organizations play a critical role in the trajectory of many individuals’ and communities’ health outcomes. By understanding this reality and grappling with what that truly means, an organization can begin the arduous task of transforming itself from simply being a part of the system, to being a partner in reforming the system in a more equitable fashion.”
As individuals, we can also have a great impact on our communities. Dawes advises five ways that we can all help eliminate health inequities on our communities:
“This is not a movement for the faint of heart,” Dawes says. “It is important to understand that we are losing money because of these health inequities—we can save $60 billion per year if we address them. We need to connect the dots to show how costly it is to exclude people, when we don’t help people reach their full potential.”
Urging people to build bridges rather than walls, Dawes recommends starting with assessments of existing policies, building networks and bridges to other communities, and illustrating the impact that current health policies have on the wellbeing of individuals, communities, and entire nations.
Voting is crucial to a healthy community, Dawes points out.
“We need leaders who care and who understand the impact of health inequities,” he says. “We need leaders who have the courage to make change and to persevere until change happens.”
“Now, more than ever, political decisions—on both sides of the aisle—are affecting our social conditions and are the root cause of our nation’s declining health,” concludes Lynn Todman. “Our hope is that this presentation will help foster new ways of thinking and cause us to consider how we can partner, build capacity, and create the change required to address the health inequities that plague American society.”
Anyone interested in learning more about structural racism and its impact on the health of communities of color is invited to join in Brave Talks, a safe, facilitated, informal gathering for six sessions. Contact by email here or visit this website.
Author

Related Articles
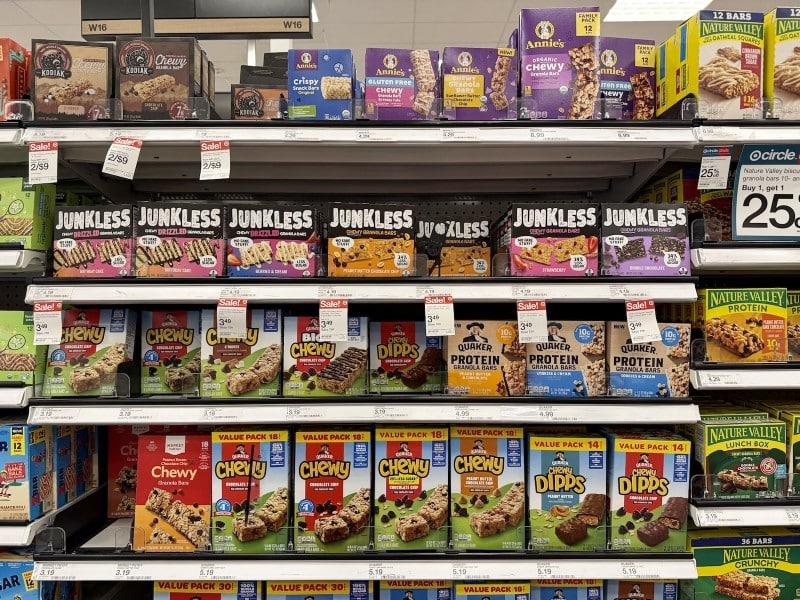
The 12-Year journey that put Junkless on grocery shelves nationwide
Former Kellogg executives Ernie Pang and Larry Beyer spent 12 years building Junkless Foods into a national granola bar brand focused on simple ingredients before selling a majority stake to Impact Capital.

A first-of-its-kind millage request on the August ballot to strengthen child care in Kalamazoo County
Kalamazoo County voters will decide in August whether to approve a first-of-its-kind child care millage that would create long-term funding to lower costs for families, support early childhood educators, and expand access to quality child care.

From cannabis to AI: Proposed Kalamazoo data center sparks questions about its future in Milwood
A proposal to convert a former Kalamazoo cannabis grow facility into an AI data center has sparked community debate over its potential impacts.