

Editor’s note: This story is part of Southwest Michigan Second Wave’s On the Ground Battle Creek series.
Elevated rates of heart disease and diabetes within Native American communities can be directly tied to the atrocities they experienced beginning in the mid-1800s, says Jamie Stuck, Tribal Chairperson of the Nottowaseppi Huron Band of the Potawatomi and newly-appointed member of a Tribal Advisory Committee that works with the U.S. Department of Health and Human Services.
“In our communities, these disparities are larger. Heart disease, diabetes, and substance abuse, a lot of that is more trauma-based as well as behavioral health,” Stuck says. “This has been going on for generations. It (started) shortly after European contact began.”
Stuck will be bringing attention to these disparities throughout his two-year appointment as the Bemidji Area Office Primary Delegate to the Advisory Committee, known as the Secretary’s Tribal Advisory Council (STAC) which was created in 2000 by Executive Order. The Bemidji Area Office for the Indian Health Service (IHS) provides service and support to 34 Federally-recognized Tribes and four Urban Indian Health programs in Illinois, Indiana, Michigan, Minnesota, and Wisconsin. Tribes in the Bemidji Area include Ojibwe (Chippewa), Ho-Chunk, Menominee, Mohican, Oneida, Odawa, Potawatomi, and Sioux.
Stuck will also be partnering and collaborating with the other 11 Indian Health Service areas, in addition to Bemidji.
“My top priority is really just to listen to tribes in the Bemidji areas,” Stuck says of his role with STAC. “I’m there to represent 34 tribes and their concerns, to provide solutions to those concerns, and be a voice for them with the people who are in control of their healthcare and the services provided. We’ve got some pretty important ears who are going to listen to what we have to say.”
Those ears belong to the leadership of the Centers for Disease Control (CDC) and the National Institutes of Health (NIH), in addition to Xavier Becerra, Secretary of the U.S. Department of Health and Human Services. These organizations have been collecting data about the health issues facing Native Americans.
The Centers for Disease Control says Native American adults are twice as likely to be diagnosed with diabetes than the general population, and that the suicide rate among Native Americans in the U.S. is more prevalent than in any other racial or ethnic group in the U.S. The CDC also says that COVID-19, heart disease, and cancer are the leading causes of death among Native Americans.
A 2022 report by the National Center for Health Statistics shows that there is a 6.5 year decline in life expectancy for Native Americans and Alaska Natives that was precipitated by the pandemic.
“This astounding figure translates to an overall drop in average living years from 71.8 years in 2019 to 65.2 by the end of 2021,” says the Stamford Advocate story.
The forward momentum of the overall declines in the health of Native Americans was generated in part by the introduction of commodity foods provided by the Federal government to Native Americans living on reservations. Stuck says there is a direct correlation between the introduction of these foods which were never meant to be part of Native American diets and the health issues that began to surface that are disproportionately impacting them.
When Native Americans were forced onto reservations, they stopped eating fresh vegetables, wild rice, game, and fish. Government commodities replaced the organic, nutrient-rich foods that had been part of their lives for hundreds of years, says Dr. Martin Reinhardt, an Anishinaabe Ojibway citizen of the Sault Ste. Marie Tribe of Chippewa Indians from Michigan and an assistant professor of Native American Studies at Northern Michigan University in Marquette.
Reinhardt has been monitoring the health of Native Americans who live in the Great Lakes Region for many years and he has known something is terribly wrong for some time, says an article in Great Lakes Now.
In March of 2012, Rheinhardt and 25 people in the Marquette area agreed they would eat only foods that grew in the Great Lakes region three hundred years ago before Europeans came to the Americas. The research project titled “The Decolonizing Diet” (DDP) was carried out through Northern Michigan University.
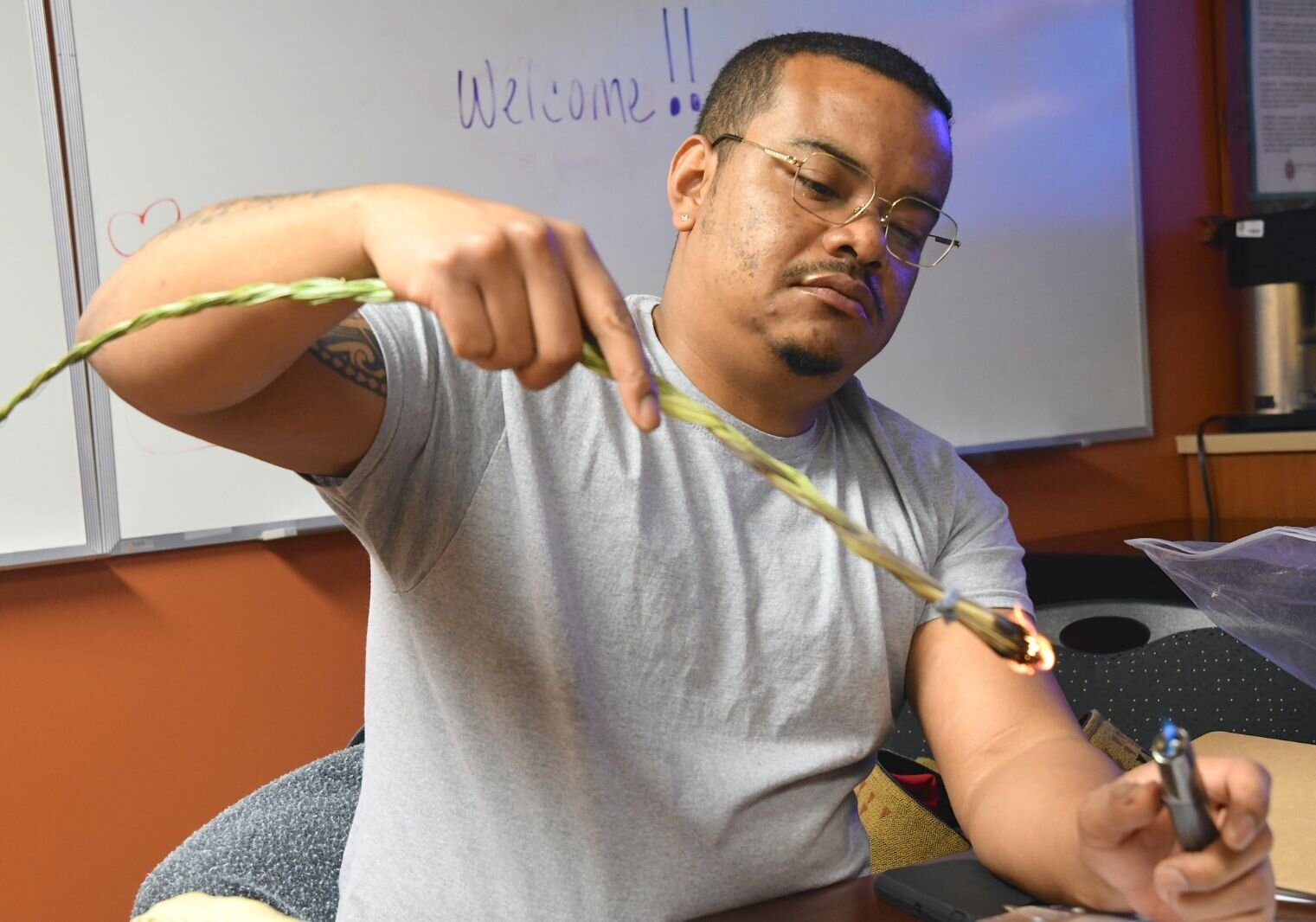
The group ate cranberries, wild rice, fish, venison, maple syrup, and other locally sourced foods, and started recreating teas and other products made from roots and herbs Reinhardt’s ancestors once gathered along the shores of the Great Lakes and deep in the forests. They also learned to make flour out of nuts, corn, and other produce and started shopping at farmer’s markets and using co-ops more than they ever had before.
The group tried this experiment for one year and got physicals and check-ups regularly as well as at the beginning and end of the trial. The information was analyzed the following year.
Reinhardt says the results were astounding. He says the health of every participant improved.
“When you have foods introduced into your diet that you’re not normally used to ingesting, it will impact your health,” Stuck says. “It’s funny how people have this idea that things like Indian Fry Bread are one of our traditional foods. It’s not because it’s nothing more than flour, baking soda, salt, and water fried in lard.”
The diet that Native Americans eat now is not the diet that they’re accustomed to, says Rosalind Johnston, NHBP Health and Human Services Director.
“We are not conditioned to eat the kind of food we are eating and that contributes to the diseases we’re dealing with now,” she says.
Health issues in his people, including obesity, high cholesterol, high blood pressure, and addiction to cigarettes, drugs, and alcohol were caused by problems created by bad nutrition, often due to lack of availability of healthy foods, Reinhardt says.
The majority of food commodities are processed and Stuck says, “This was all part of a campaign to break down the family structure. When we were forced to go to boarding schools and reservations it was a breakdown of our way of life.”
In addition to the major changes in diet, Reinhardt says he also wondered if some of the issues were caused by a separation from a culture that was taken away from them. This separation resulted in generational trauma that has been passed down.
This trauma is an element that healthcare providers need to be aware of and address when treating Native American patients, Johnston says. NHBP has two health clinics – one on the Pine Creek Indian Reservation in Athens and another in Grand Rapids – that offer primary care, dental, behavioral health, maternal child visits, transportation services, nutrition, and fitness.
“The healthcare providers at our clinics are trained in trauma-informed practice. They have to understand the history and trauma of the tribe; adverse childhood effects and what that means in terms of their practice and they have to be able to acknowledge that there is a story that impacted those individuals coming in through their doors,” Johnston says. “They are developing relationships that are patient-centered and giving information and encouraging the patient to achieve their goals. Our visits are anywhere from 30 minutes to one hour.”
Incorporating this culturally appropriate approach into healthcare for Native Americans is among the issues Stuck will be focusing on with the Tribal Advisory Committee.
He cites a healthcare model used in Alaska that allows patients to be more involved with their treatment options and the methods used. He says it’s critical to have a support system, like a spouse or partner, in there with patients so it doesn’t come down to the healthcare provider saying, “This is how we’re going to do it.”
“Taking more of a culturally sensitive approach to things makes indigenous people a little more comfortable,” Stuck says. “In my opinion, I believe that since tribes are sovereign entities there’s more of an opportunity to really focus on the prevention aspects of health versus treating the disease.”
Lived experience
As Chairperson of NHBP, Stuck actively oversees the NHBP’s healthcare programs serving 3,500 people, says Dorie Rios, NHBP Tribal Vice Chairperson, in her nomination of Stuck to the Tribal Advisory Committee. She says Stuck has also served as Chair of the Tribe’s Journey to Wellness Committee since 2010 and chairs NHBP’s Health Compliance Board, which assists the Tribe in fulfilling its compliance responsibilities. Like the vast majority of the Tribal nations within the Bemidji Area, NHBP operates its healthcare clinics through self-governance compacts with the Indian Health Service.
“While his efforts target taking care of his own citizens, Stuck also looks at the bigger picture of how Native Americans receive health services and are counted within the systems that track their data,” says Elizabeth Hertel, director of the Michigan Department of Health and Human Services, in a press release about Stuck’s appointment. “He has helped the Michigan Department of Health and Human Services to turn our focus to improving the quality of data related to Native American populations and ways we can better share that data with Tribal Governments and our Urban Indian Organization providing health care in the metropolitan Detroit area.”
Currently, Native Americans don’t have their own box to check on healthcare forms to indicate tribal affiliation. Stuck says this makes the collection of accurate data difficult.
“We really need to find a way to improve Native American data collection. We’re not getting the full story because of shortfalls in surveying and getting data that end up being lumped in with the ‘Other’ category,” Stuck says. “There isn’t a connection to their tribe or affiliation. The state of Michigan should have the means to make a specific box that Native Americans can check that will be part of the surveying option on these forms. It’s important to know what the tribal affiliation is.”
Healthcare on their terms
The clinics in Athens and Grand Rapids serve NHBP tribal members in addition to any American Indian or Alaska Native, Johnston says. There’s no cost for the services.
“Eligibility has been expanded so we can see state-recognized Native Americans, for example, members of the Grand River Tribe,” she says. “We also see individuals of First Nations, so they might be from First Nations in Canada, but live in the United States.”
Residents of Athens, East Leroy, Fulton, and Union City also can receive healthcare services through the NHBP clinic on the Pine Creek Reservation. They are billed for those services, Johnston says.
“There’s very little primary care available to them that’s local,” she says. “This is something the Tribe is doing to give back to surrounding communities.”
Stuck says Athens residents can come into the Pine Creek Reservation clinic. The NHBP has a third on-site health clinic for employees of FireKeepers Casino. Johnston says this clinic focuses on primary care and occupational health.
“Oftentimes in healthcare, access is an issue,” she says. “If you are able to provide access to individuals that’s convenient to them, they’re more likely to see you rather than ending up in urgent care or the emergency room, which is keeping employees and saving money for the Casino.”
Because the clinics are established within Native American communities and there is consistency in healthcare providers, Johnston says tribal members know that the clinics are a “culturally appropriate place. They see traditional medicine practiced and see artwork that they can connect to. They’re not afraid to come into our clinics. Are they afraid to seek healthcare from other organizations? That’s a possibility.”
While intentional efforts are made to create clinics that reflect the traditions and customs of Native American communities, Johnston and Stuck both say there is a shortage of healthcare providers who identify as Native Americans.
Out of the estimated more than 5.2 million American Indians and Alaska Natives (AI/ANs) in the U.S., about 3,400 are physicians, just 0.4% of the physician workforce, according to a 2018 AMA Council on Medical Education report, “Study of Declining Native American Medical Student Enrollment,” says an article on the American Medical Association website.
“Western Michigan University has noticed this as an issue in Southwest Michigan and they’re really engaging Native American people to get into the medical profession,” Stuck says. “It takes time for our people to build trust. Our health and our lives are a high priority for us. It takes a special person to work in Indigenous communities. For them, it has to be about more than a paycheck and they are here because they want to be.”
Johnston says Tribal health clinics are competing with hospital systems to recruit and retain physicians, both Native American and non-Native American.
“One of the things we look at is growing our own pipeline of physicians and other healthcare providers. We know it is really hard to recruit professionals to work in an environment that has a very different focus than mainstream healthcare,” Johnston says. “It’s not bottom-line driven, it’s people-driven. Those who come to work at Indian health clinics have to want to sit into this environment.”
Stuck says this is another priority area for him as a STAC delegate. He says he’s not content to be little more than a mouthpiece for the Tribes he represents.
“I expect them to listen to my comments and not just check off the box,” Stack says of his message to other STAC participants. “I want them to entertain my discussions and solutions and what my people are dealing with. You can’t just put us into one large category.”
Author

Related Articles

Sustainability is everywhere on campus — so why do students feel left behind?
As colleges promote sustainability through recycling programs and climate initiatives, students and faculty at Kalamazoo College and Western Michigan University question whether higher education institutions are doing enough to address the climate crisis through funding, policy, and climate education.

Battle Creek Battle Jacks sold: New owner Scott Miles plans new era for team
The Battle Creek Battle Jacks enter a new era under owner Scott Miles, a Massachusetts businessman investing in fan experience, community engagement, and competitive summer collegiate baseball in the Northwoods League.

Kalamazoo and Calhoun County seniors helped to age-in-place through Milestone’s home-repair program
Milestone Senior Services helped an Oshtemo senior replace a failed furnace and rebuild an unsafe ramp at no cost through grant-funded home repair and accessibility programs serving Kalamazoo and Calhoun counties.